DATA ANALYSIS
Crime Data
The 2025 IAHSS Foundation Healthcare Crime Survey presents an analysis of crime and security incident data reported by participating facilities for calendar year 2024. A total of 193 survey responses were received, consistent with recent survey cycles. Following data validation, 182 responses were deemed usable. As in prior years, a response was considered usable when the facility reported its licensed bed count and submitted the majority of core crime metrics, as these elements are essential for calculating reliable, exposure-adjusted rates.
The findings presented in this section reflect incidents occurring during the 2024 reporting period. Crime rates were calculated as incidents per 100 licensed beds, using the formula (Incidents ÷ Licensed Beds) × 100, to support standardized benchmarking and comparability across facilities of varying size, service mix, and patient population. In select analyses, adjusted rates were used to mitigate the influence of zerobed facilities and statistical outliers, consistent with prior survey methodology.
This approach aligns with IAHSS Healthcare Security Industry Guidelines 01.05.01 Security Incident Reporting, 01.05.02 Incident Categories and Data Analysis, and 01.05.03 Security Metrics, which emphasize standardized data collection, normalized rate analysis, and longitudinal trending to support program evaluation, benchmarking, and performance improvement. The categorization of incidents reflects the IAHSS Incident Category and Data Collection Framework, which provides a structured and consistent approach to classifying healthcare security events.
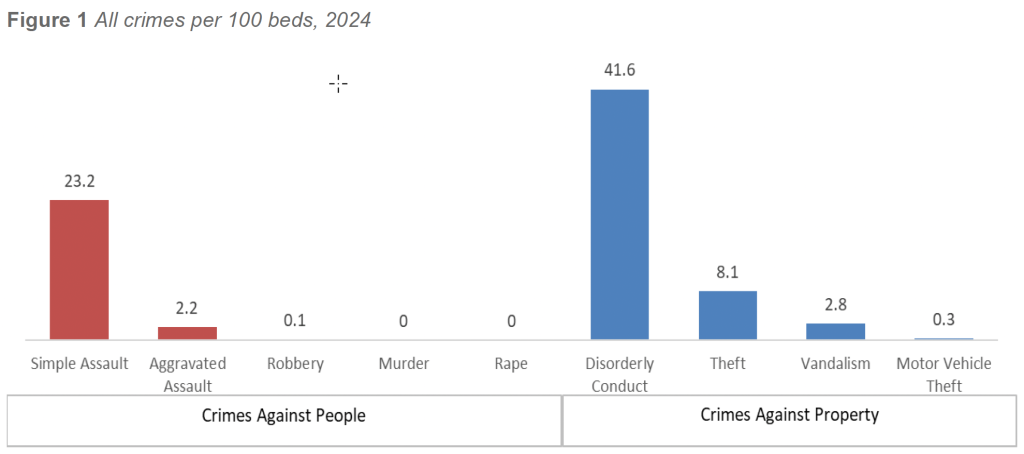
The 2024 findings reaffirm that behavior-driven and interpersonal incidents continue to dominate the security landscape in healthcare facilities. Other (Simple) Assault remained the most frequently reported crime against persons, with a weighted rate of 22.9 incidents per 100 beds. Disorderly Conduct, a category capturing behavioral escalation, agitation, and disruptive conduct, reached 41.28 incidents per 100 beds, exceeding all other reported crime categories. Together, these two categories account for the majority of crime-related activity occurring within healthcare facilities.
Traditional property crimes continued their multi-year decline. Theft remained the most frequently reported property offense at 8.06 incidents per 100 beds, followed by Vandalism at 2.82, Motor Vehicle Theft at 0.25, and Burglary at 0.17 incidents per 100 beds. Collectively, property crimes accounted for approximately 11 incidents per 100 beds, underscoring the sustained reduction of traditional criminal activity within healthcare environments.
Violent felonies remained exceedingly rare in 2024. Weighted rates for Murder (0.01), Rape (0.02), and Robbery (0.06) per 100 beds were negligible across reporting facilities. Aggravated Assault, while substantially less frequent than simple assault, remained an important operational concern at 2.18 incidents per 100 beds, particularly in higher-acuity environments and facilities with significant emergency department volume or behavioral health exposure.
The longitudinal dataset collected through the IAHSS Foundation Healthcare Crime Survey illustrates how facility crime patterns have evolved over time. Figure 2 presents weighted crime rates per 100 licensed beds for major crime categories reported between 2012 and 2024, enabling year-over-year comparison and trend analysis.
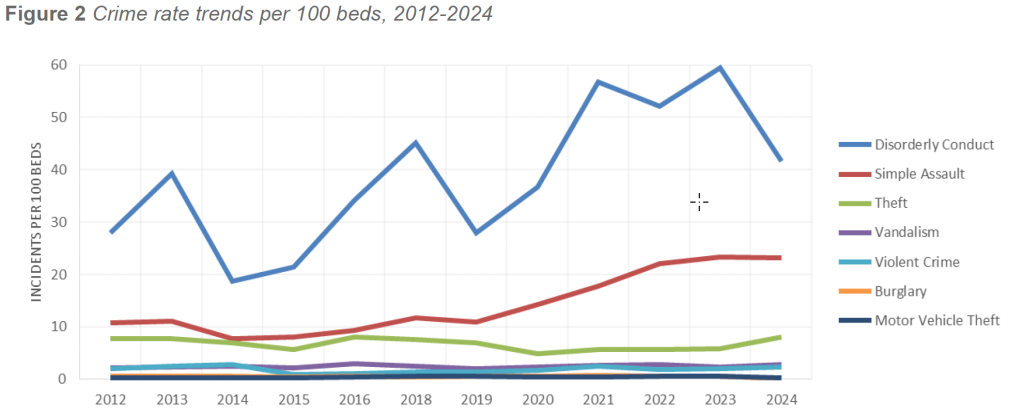
The 12-year trend line highlights several key and sustained shifts:
- Growth in behavioral and interpersonal incidents
Rates of Simple Assault and Disorderly Conduct increased substantially over the past decade, particularly between 2016 and 2022. These categories reflect rising behavioral health acuity, substance use, social instability, and emotional distress that frequently manifest in emergency departments, public-facing areas, and high-activity clinical settings. - Stabilization of serious violence
Aggravated Assault and other violent felonies increased modestly between 2019 and 2022 but have stabilized since 2023. This plateau may reflect maturation of threat management practices, behavioral response protocols, and sustained organizational investment in WPV prevention and mitigation. - Decline in property crime
Theft, Burglary, and Motor Vehicle Theft have steadily declined since 2017. Continued investments in surveillance coverage, access control, parking security, and asset-protection technologies appear to have produced durable reductions in traditional property crime exposure. - Relative stability in vandalism
Vandalism rates have fluctuated minimally year over year, suggesting persistent environmental and external pressures rather than meaningful changes in offender behavior or facility type.
Taken together, the 2024 findings and the broader historical dataset present a consistent and evolving narrative regarding healthcare facility risk. Crime exposure has shifted away from traditional property offenses toward behavior-driven, interpersonal, and clinically influenced incidents. While violent felonies remain rare, the persistence of aggravated assaults reinforces the need for structured threat management, interdisciplinary collaboration, and proactive WPV mitigation strategies.
Overall, the data confirm that the primary security burden in healthcare facilities is now rooted in behavioral and interpersonal risk rather than conventional criminal activity. This shift necessitates security strategies centered on incident reporting fidelity, data-driven analysis, clinical partnership, staffing alignment, and evidence-based WPV prevention—consistent with IAHSS guidance for modern healthcare security programs.
Workplace Violence Typology
To further characterize the nature of assaults occurring in healthcare environments, the 2024 survey asked participating facilities whether they classify WPV incidents using the Workplace Violence Typology framework. The WPV Typology categorizes violent events into four primary types based on the relationship between the perpetrator and the workplace:
- Type 1: Violence committed by individuals with no legitimate relationship to the facility
- Type 2: Violence directed at staff by patients, visitors, or others receiving services
- Type 3: Violence between current or former employees
- Type 4: Violence involving individuals with a personal relationship to an employee but no direct connection to the facility
Use of WPV Typology is a recognized indicator of organizational maturity and aligns with regulatory and industry expectations for structured incident reporting and analysis. Its application is supported by IAHSS Healthcare Security Industry Guidelines 01.05.01 Security Incident Reporting and 01.05.02 Incident Categories and Data Analysis, which emphasize consistent classification of incidents to support trend analysis, benchmarking, and prevention planning
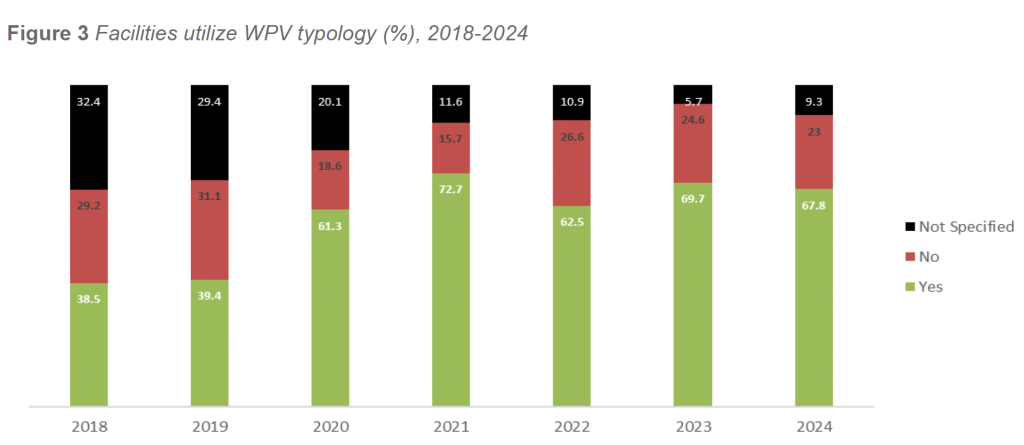
In 2024, 67.8 percent of responding facilities reported using the WPV Typology to classify assaults. This represents a slight decline from 2023 (71.0 percent) but remains consistent with the stabilization observed over the past several survey cycles. After a period of steady growth, typology adoption appears to have plateaued, suggesting that most facilities with sufficient infrastructure and analytic capacity have institutionalized typology-based reporting. Facilities not using the typology continue to be disproportionately smaller or more resource constrained. Among facilities that reported using WPV Typology, the distribution of assault types remained highly consistent with prior years.
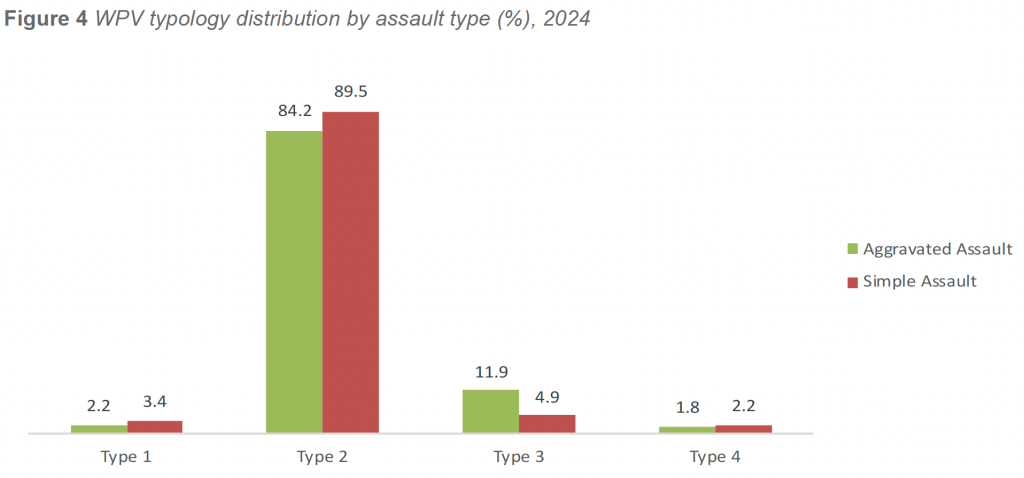
In 2024, Type 2 WPV continued to overwhelmingly define healthcare violence. Facilities reported that 84.2 percent of aggravated assaults and 89.5 percent of simple assaults were classified as Type 2 events. This pattern reinforces the clinical and behavioral realities of healthcare delivery, particularly in emergency departments, inpatient behavioral health settings, and other high-acuity, high-contact environments.
The remaining typology categories represented substantially smaller proportions of total assaults:
- Type 3 (Worker-on-Worker) incidents accounted for 11.9 percent of aggravated assaults and 4.9 percent of simple assaults, reflecting persistent but relatively low levels of interpersonal conflict within healthcare workforces.
- Type 1 (No Relationship to Facility) incidents represented 2.2 percent of aggravated assaults and 3.4 percent of simple assaults, indicating that external criminal activity remains a minor contributor to overall WPV exposure.
- Type 4 (Personal or Domestic Relationship) incidents were the least common, comprising 1.8 percent of aggravated assaults and 2.2 percent of simple assaults.
Across the 2021–2024 period, several WPV typology patterns have remained stable:
- Type 2 incidents consistently account for the vast majority of assaults, generally exceeding 80–90 percent annually.
- Type 3 incidents remain low but persistent, reflecting ongoing interpersonal pressures in highstress clinical environments.
- Type 1 and Type 4 incidents remain rare, together accounting for less than 10 percent of all assaults in any given year.
- Typology adoption has stabilized, indicating that structured WPV classification has become embedded in facilities with more mature security and reporting programs.
The consistent dominance of Type 2 WPV underscores that violence in healthcare is behavior-driven, clinically influenced, and structurally predictable, rather than random or externally driven. This finding aligns with IAHSS Healthcare Security Industry Guideline 01.09 Violence in Healthcare, which emphasizes the need for multidisciplinary prevention strategies addressing patient- and visitorgenerated aggression through early identification, de-escalation, environmental controls, and coordinated response processes.
Overall, WPV Typology remains a critical analytic tool for healthcare security programs. Facilities that consistently apply typology-based classification are better positioned to monitor trends, allocate resources, justify staffing and training models, and advance formal WPV prevention and threat management initiatives. The continued stability of typology patterns across multiple years reinforces both the validity of the framework and its value in guiding data-driven mitigation strategies.
WPV Typology by Behavioral Health Facility Type
To further contextualize WPV exposure across healthcare environments, 2024 WPV typology results were examined separately for facilities with inpatient psychiatric/behavioral health units and facilities without BH units. Rates are expressed as incidents per 100 licensed beds, allowing for standardized comparison across facility types.
This analysis aligns with IAHSS Healthcare Security Industry Guidelines 01.05.02 Incident Categories and Data Analysis and 01.05.03 Security Metrics, which emphasize the use of normalized rates and stratified analysis to identify meaningful differences in WPV exposure and inform targeted prevention strategies.
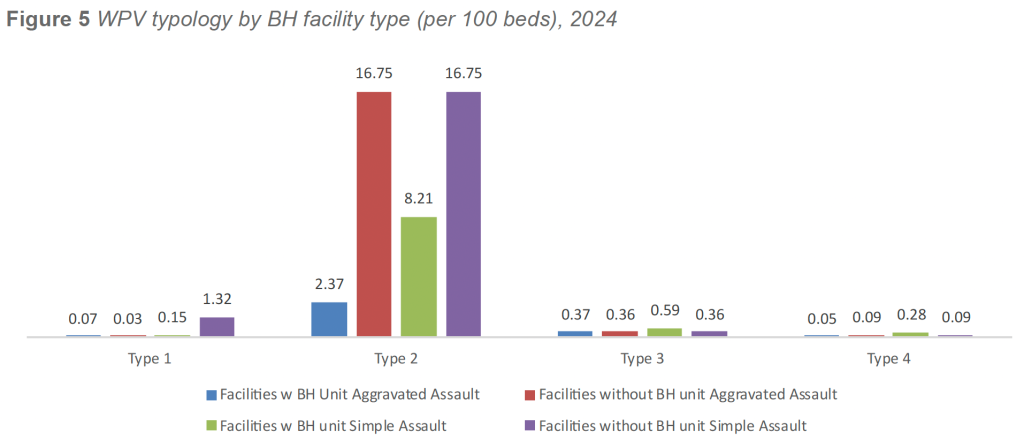
Type 2 (Patient- or Visitor-on-Worker) Assaults
In 2024, Type 2 aggravated assault rates were lower in facilities with BH units, averaging 2.37 incidents per 100 beds, compared with 16.7 incidents per 100 beds in facilities without BH units. A similar pattern was observed for Type 2 simple assaults, with facilities operating BH units averaging 8.21 incidents per 100 beds, compared with 16.75 incidents per 100 beds in facilities without BH units.
The higher concentration of Type 2 assaults in non-BH facilities highlights the operational challenges associated with managing behaviorally complex or psychiatric patients in environments not specifically designed for inpatient behavioral health care, such as emergency departments, medical-surgical units, and observation areas.
Type 3 (Worker-on-Worker) Assaults
Type 3 assault rates were comparable across facility types. Aggravated Type 3 assaults averaged 0.37 incidents per 100 beds in facilities with BH units and 0.36 incidents per 100 beds in facilities without BH units. Simple Type 3 assaults followed a similar pattern, averaging 0.59 incidents per 100 beds in facilities with BH units and 0.36 incidents per 100 beds in facilities without BH units.
These findings suggest that worker-on-worker WPV is influenced less by the presence of inpatient behavioral health services and more by universal factors such as operational stress, staffing pressures, and the high-intensity nature of healthcare work environments.
Type 1 (No Relationship to Facility) Assaults
Type 1 incidents remained infrequent across both facility types. Facilities with BH units reported slightly higher aggravated Type 1 assault rates at 1.09 incidents per 100 beds, compared with 0.07 incidents per 100 beds in facilities without BH units. Conversely, simple Type 1 assaults were marginally lower in facilities with BH units (2.31 incidents per 100 beds) compared with facilities without BH units (2.98 incidents per 100 beds).
Although these differences are modest, the overall low volumes reinforce that external criminal activity is not a primary driver of WPV in healthcare settings.
Type 4 (Personal or Domestic Relationship) Assaults
Type 4 incidents were more prevalent in facilities with BH units. Aggravated Type 4 assaults averaged 0.88 incidents per 100 beds in facilities with BH units, compared with 0.07 incidents per 100 beds in facilities without BH units. Simple Type 4 assaults demonstrated a similar pattern, with facilities operating BH units averaging 4.65 incidents per 100 beds, compared with 0.20 incidents per 100 beds in facilities without BH units.
While Type 4 incidents remain rare overall, their elevated presence in facilities with BH units reflects added interpersonal, psychosocial, and situational complexity within these environments, including the intersection of personal relationships, behavioral health treatment, and workplace stressors.
Summary and Implications
Collectively, the 2024 WPV typology data demonstrate meaningful differences in WPV exposure based on the presence or absence of inpatient behavioral health services. Facilities without BH units experienced higher rates of Type 2 patient- or visitor-generated assaults, underscoring the risks associated with managing behaviorally complex patients in non-specialty settings. At the same time, facilities with BH units exhibited higher rates of Type 4 incidents and modestly higher Type 1 aggravated assaults, reflecting the broader interpersonal and psychosocial dynamics present in behavioral health environments.
Consistent with IAHSS Healthcare Security Industry Guideline 01.09 Violence in Healthcare, these findings reinforce that WPV is behavior-driven, clinically influenced, and structurally predictable, rather than random. The data highlight the importance of aligning staffing models, environmental design, deescalation capabilities, and multidisciplinary threat management processes with the specific risk profile of each facility type.
WPV typology remains an essential analytic tool for distinguishing these patterns and guiding targeted prevention strategies. Facilities that consistently apply typology-based analysis are better positioned to identify emerging risks, allocate resources appropriately, and advance comprehensive, data-driven WPV prevention programs.
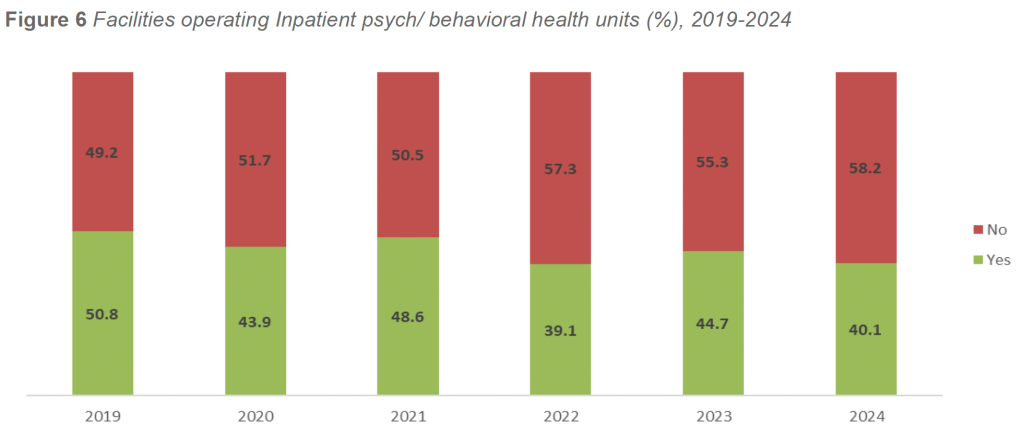
Inpatient Psychiatric/Behavioral Health Units
To further examine the relationship between inpatient behavioral health capacity and security incident patterns, the 2024 survey asked facilities whether they operate an inpatient psychiatric or behavioral health unit. These units represent some of the highest-acuity environments in healthcare and are associated with unique clinical, behavioral, and security challenges that directly influence WPV exposure and overall incident volume.
This analysis aligns with IAHSS Healthcare Security Industry Guideline 05.07 Behavioral / Mental Health – General, which recognizes inpatient behavioral health environments as presenting elevated risks related to patient aggression, self-harm, interpersonal violence, and security resource utilization, as well as Guideline 01.04 Security Vulnerability Assessments, which emphasizes the importance of accounting for patient population complexity when evaluating security risk.